How is dystocia diagnosed
Fetal dystocia is abnormal fetal size or position resulting in difficult delivery. Diagnosis is by examination, ultrasonography, or response to augmentation of labor. Treatment is with physical maneuvers to reposition the fetus, operative vaginal delivery.
Can you see shoulder dystocia on ultrasound?
Several previous studies have shown that prenatal sonographic findings can predict shoulder dystocia at term in diabetic mothers, but this appears to be the first study of elective third-trimester sonography in low-risk nondiabetic women, the investigators noted.
Can shoulder dystocia be predicted?
CAN SHOULDER DYSTOCIA BE PREDICTED? There is expert consensus that the occurrence of shoulder dystocia cannot be accurately predicted by antenatal or intrapartum risk factors or imaging studies [2].
What are some signs of shoulder dystocia?
Shoulder dystocia is when, after vaginal delivery of the head, the baby’s anterior shoulder gets caught above the mother’s pubic bone. Signs include retraction of the baby’s head back into the vagina, known as “turtle sign”. Complications for the baby may include brachial plexus injury, or clavicle fracture.Where do they cut for episiotomy?
An episiotomy is a cut (incision) through the area between your vaginal opening and your anus. This area is called the perineum. This procedure is done to make your vaginal opening larger for childbirth.
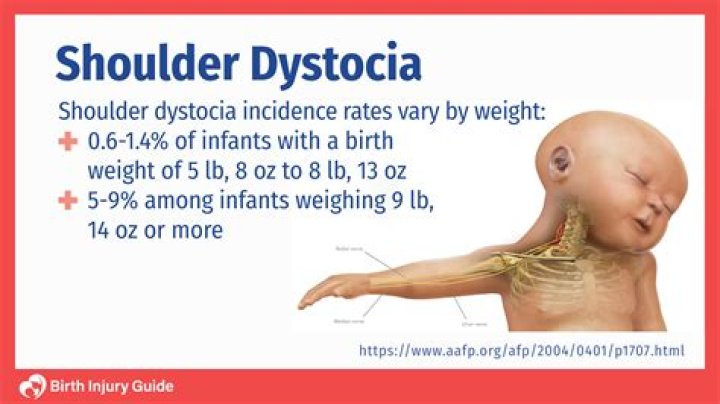
What percentage of babies 4 kg make up cases of shoulder dystocia?
Half of all instances of shoulder dystocia occur in babies weighing less than 4 kg (about 9 lb). Ultrasound scans are not good at telling whether you are likely to have a large baby and therefore they are not recommended for predicting shoulder dystocia, if you have no other risk factors.
What is fetal distress?
Fetal distress is a sign that your baby is not well. It happens when the baby isn’t receiving enough oxygen through the placenta. If it’s not treated, fetal distress can lead to the baby breathing in amniotic fluid containing meconium (poo).
What is the most common injury to the baby following a shoulder dystocia?
Brachial plexus injury to the newborn is the most common complication of shoulder dystocia. Most of these injuries resolve before discharge from the hospital.Can babies survive shoulder dystocia?
Most babies recover from shoulder dystocia very well. But because they may have been injured or deprived of oxygen, they may need to be watched more closely or spend time in the neonatal intensive care unit. Some babies will need physiotherapy, and you may need help with breastfeeding if your baby has been injured.
Is shoulder dystocia an emergency?Shoulder dystocia is an obstetric emergency in which normal traction on the fetal head does not lead to delivery of the shoulders. This can cause neonatal brachial plexus injuries, hypoxia, and maternal trauma, including damage to the bladder, anal sphincter, and rectum, and postpartum hemorrhage.
Article first time published onCan you sue for shoulder dystocia?
Almost all shoulder dystocia malpractice suits imply that the delivery was mishandled by the obstetrician or midwife. By far the most common type of injury leading to suit is a brachial plexus injury, resulting in some degree of permanent paralysis of one or both shoulders, arms, or hands of the infant.
Is shoulder dystocia life threatening?
A condition known as shoulder dystocia might occur during birth. This is a potentially life-threatening issue that must be properly addressed. Shoulder dystocia means that the baby’s shoulders get stuck in the mother’s pelvis during birth. The head is delivered but the shoulders are stuck.
Which patient is at highest risk for shoulder dystocia?
- Macrosomia. …
- Having preexisting diabetes or gestational diabetes. …
- Having shoulder dystocia in a previous pregnancy.
- Being pregnant twins, triples or other multiples.
- Being overweight or gaining too much weight during pregnancy.
How do you deliver a shoulder dystocia?
Because most cases of shoulder dystocia can be relieved with the McRoberts maneuver and suprapubic pressure, many women can be spared a surgical incision. This procedure involves flexing and abducting the maternal hips, positioning the maternal thighs up onto the maternal abdomen.
What is the biggest risk factor for shoulder dystocia?
Shoulder dystocia and brachial plexus injury occur in 0.5% to 1.5% of all births. Risk factors for both include maternal obesity, excessive prenatal weight gain, maternal diabetes, protracted labor, and fetal macrosomia.
Why do doctors cut vagina during birth?
Doctors do an episiotomy to make it easier for the baby’s head to pass through for delivery and to prevent complications or a vaginal tear. This cut is made during the second stage of labor right before the baby’s head is delivered. 2 After the baby is born, the doctor uses stitches to repair the incision.
What is median episiotomy?
An episiotomy is an incision made in the perineum — the tissue between the vaginal opening and the anus — during childbirth. A midline (median) incision (shown at left) is done vertically. A mediolateral incision (shown at right) is done at an angle.
Can you feel yourself tear during birth?
It is very uncommon for women to actually feel themselves tearing, due to the intensity and pressure that occurs during this stage of labour. Often women will be told they have a small graze or tear and express surprise as they didn’t feel it happening.
What is thick meconium?
Meconium is a thick, green, tar-like substance that lines your baby’s intestines during pregnancy. Typically this substance is not released in your baby’s bowel movements until after birth. However, sometimes a baby will have a bowel movement prior to birth, excreting the meconium into the amniotic fluid.
Do contractions affect the baby heart rate?
Heart rate increases during contractions. Heart rate returns to normal after baby moves or after a contraction. Your contractions are strong and regular during labor.
How would you know if your baby is in distress?
- Decreased movement by the baby in the womb.
- Cramping.
- Vaginal bleeding.
- Excessive weight gain.
- Inadequate weight gain.
- The “baby bump” in the mother’s tummy is not progressing or looks smaller than expected.
Does C Section prevent shoulder dystocia?
Shoulder dystocia often causes brachial plexus, an injury to the nerves that control the shoulder, arm, hands and fingers. In their study, Hankins and his colleagues found that elective C-sections at 39 weeks reduce the risk of shoulder dystocia. Risk factors for shoulder dystocia include: Fetal macrosomia (large baby)
At what point during a pregnancy does shoulder dystocia become evident?
Shoulder dystocia commonly occurs at stage 2, where the anterior shoulder becomes impacted on the maternal pubic symphysis.
Can an epidural cause shoulder dystocia?
Use of epidural anesthesia was associated with an increased risk for shoulder dystocia (odds ratio = 3.47, 95% confidence interval [2.72, 4.42]).
Can baby get too big for uterus?
Risks associated with fetal macrosomia increase greatly when birth weight is more than 9 pounds, 15 ounces (4,500 grams). Fetal macrosomia may complicate vaginal delivery and can put the baby at risk of injury during birth. Fetal macrosomia also puts the baby at increased risk of health problems after birth.
What if I cant push my baby out?
Even though you may be pushing with all the strength you can muster, your energy may have waned, and because of fatigue, your pushing may not be strong enough to deliver the baby. Alternatively, it may be a tight fit or the baby may need to be rotated to a better position in order to squeeze out.
What is shoulder dystocia death?
In a year, shoulder dystocia is experienced by more than 20,000 women during delivery in the United States and gives rise to a host of health problems to both the mother and the baby. In fact, shoulder dystocia is considered as a medical emergency as fetal death can occur due to compression of the umbilical cord.
How many bones break during delivery?
There were 35 cases of bone injuries giving an incidence of 1 per 1,000 live births. Clavicle was the commonest bone fractured (45.7%) followed by humerus (20%), femur (14.3%) and depressed skull fracture (11.4%) in the order of frequency.
Which maneuver is first attempted to deliver an infant with shoulder dystocia?
The McRoberts Maneuver is often attempted first because it is simple and effective. In fact, the McRoberts maneuver has been found to single-handedly resolve between 39% and 42% of shoulder dystocia cases.
When the fetal shoulders fail to deliver spontaneously Who is at risk?
Failure of the shoulder to delivery spontaneously places both the pregnant woman and fetus at high risk for permanent birth-related injury (1). Brachial plexus injuries are one of the most important fetal complications of SD, complicating 4–16% of such deliveries (7).
Can babies get stuck in one position?
Favoring this position close to delivery is relatively rare. In fact, only around one out of every 500 babies settle into a transverse lie in the final weeks of pregnancy. This number could be as high as one in 50 before 32 weeks gestation.