What is G tube malfunction
Peristomal leakage. Ulceration. Gastric outlet obstruction. Inadvertent gastrostomy tube removal. Leakage of gastric contents or tube feeds into the peritoneal cavity.
What is the cause of gastrostomy?
Reasons for Procedure A gastrostomy is needed if food cannot pass through the mouth and throat. It may be needed to feed a person that has: A hard time swallowing. Severe eating problems.
What is the most common cause of gastrostomy tube blockage?
- Poorly crushed medications.
- Not flushing gastrostomy tube when feeds are completed.
- Feed too thick or containing lumps of powder.
- Vitamised food being put down tube.
- Leaving formula in the tube to curdle.
What happens if G tube is placed wrong?
An incorrectly positioned external flange will allow the internal bumper to come away from the stomach wall and leakage can occur. An incorrectly placed external fixation plate – more than 0.5cm from the skin – will allow the tube to move in and out of the stoma and gastric content to leak out of the stoma.What is gastrostomy feeding?
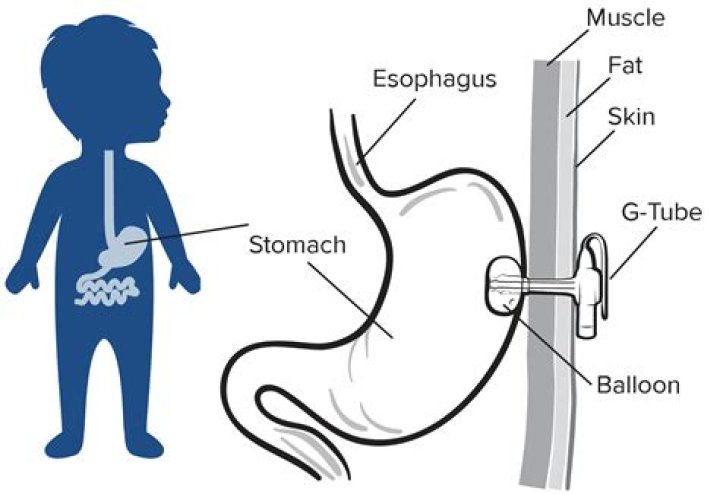
A gastrostomy is a surgical procedure used to insert a tube, often referred to as a “G-tube”, through the abdomen and into the stomach. Gastrostomy is used to provide a route for tube feeding if needed for four weeks or longer, and/or to vent the stomach for air or drainage.
How is gastrostomy done?
Gastrostomy feeding tube (G-tube) insertion is done in part using a procedure called endoscopy. This is a way of looking inside the body using a flexible tube with a small camera on the end of it. The endoscope is inserted through the mouth and down the esophagus, which leads to the stomach.
Why would a child need a gastrostomy?
A gastrostomy can be helpful for anyone who needs long term support with feeding or to receive extra nutrients to grow and develop. Some children and young people have a neurological (nervous system) disorder that affects their swallowing which increases the chance of breathing in food (aspiration).
What is the most common problem in tube feeding?
Diarrhea. The most common reported complication of tube feeding is diarrhea, defined as stool weight > 200 mL per 24 hours.Is gastrostomy a major surgery?
Percutaneous endoscopic gastrostomy (PEG) tube placement procedure is not a major surgery. It does not involve opening the abdomen.
Can an RN replace a G tube?A: Carol McGinnis, RN, MS, CNSC, replies: Replacing a gastrostomy tube is within the scope of practice of registered nurses on a state-specific basis. Thus, it is important to review your state’s nurse practice act in this regard.
Article first time published onHow do you confirm G tube placement?
Before the G-tube is used for feedings, placement must be confirmed. Classically, confirmation is achieved by injecting 20-30 mL of water-soluble contrast solution (diatrizoate meglumine diatrizoate sodium) into the tube and taking a supine abdominal radiograph within 1-2 minutes.
What is the life expectancy of a person with a feeding tube?
For the 216 remaining patients, life expectancy without the feeding tube was a median of 1–2 months and it increased to an anticipated life expectancy of a median of 1–3 years with the feeding tube in place.
How long can you live with a PEG tube?
There is some evidence to suggest that PEG tubes may decrease mortality among specific subgroups, such as those with ALS (13). Approximately 81% of all patients survived 30 days after PEG placement, and 38% were alive at 1 year.
How do I know if my G tube is infected?
Signs of infection include: redness, foul smelling discharge, green thick or white discharge, swelling around the feeding tube, abscess formation, pinpoint rash, pain and fever.
What is venting gastrostomy?
Venting gastrostomy (VG) is an alternative to both prolonged medical therapy with nasogastric intubation and intestinal bypass/diversion for refractory MBO. Limited published data from large academic research centers support use of VG in patients with advanced ovarian cancer and MBO.
What is Stamm gastrostomy?
The Stamm gastrostomy is an open technique, requiring an upper midline laparotomy and gastrotomy, with the catheter brought out in the left hypochondrium. It was first devised in 1894 by the American Gastric Surgeon, Martin Stamm (1847–1918), who was educated greatly in surgery when he visited Germany.
How do you feed a gastrostomy?
- Attach a 60cc syringe to the end of your feeding tube.
- Pull back on the plunger. You should see some gastric juices (yellow-green fluid). …
- If you pull back a large amount of fluid, do not give yourself food. Inject the stomach content, which contains important minerals, back into the tube.
How do you unclog a feeding tube with pancreatic enzymes?
If tube is still blocked, PLACE pancreatic enzyme tablet and sodium bicarbonate tablet into pill crusher and crush tablets into fine powder. Transfer powder to med cup and ADD 4 mL of warm water (or sterile water) to dissolve thoroughly. Additional water may be added if required.
Which patient is most likely at risk of refeeding syndrome?
Who is at risk of developing refeeding syndrome? People at risk include patients with protein-energy malnutrition, alcohol abuse, anorexia nervosa, prolonged fasting, no nutritional intake for seven days or more, and significant weight loss.
What are the complications of tube feeding?
- Constipation.
- Dehydration.
- Diarrhea.
- Skin Issues (around the site of your tube)
- Unintentional tears in your intestines (perforation)
- Infection in your abdomen (peritonitis)
- Problems with the feeding tube such as blockages (obstruction) and involuntary movement (displacement)
Who needs gastrostomy tube?
Who Needs a G-Tube? Kids need G-tubes for different kinds of health problems, including: congenital (present at birth) problems of the mouth, esophagus, stomach, or intestines. sucking and swallowing disorders (due to premature birth, injury, a developmental delay, or another condition)
How long does it take for a gastrostomy to heal?
If your child has a stitch around the tube, healing takes place in about 21 days. A tract will form between the stomach and skin in about three months. Your doctor may talk to you about changing the tube at this time. It is important to know what type and size tube your child has.
How often should a gastrostomy tube be changed?
Balloon G tubes should be changed at least every six to eight months to prevent the balloon from leaking or breaking which can cause the G tube to accidentally fall out. The G tube feeding extension set should be changed every month.
Is a gastrostomy safe?
Percutaneous endoscopic gastrostomy (PEG) is a relatively safe procedure; however, acute and chronic complications of PEG have been reported. We aimed to determine risk factors associated with complications and 30-day mortality after PEG, based on 11 years of experience at a single tertiary hospital.
What are the risks of PEG feeding?
- Reactions to the anesthesia.
- Pain.
- Leakage of stomach contents around the tube.
- Infection of the tube site.
- Infection that spreads inside the belly.
- Aspiration.
- Bleeding from the incision area.
- Bleeding or infection from damage to other organs inside the belly.
What different types of gastrostomy are there?
There are two common types of gastrostomy, Percutaneous Endoscopic Gastrostomy devices (PEGS) and low-profile ‘Buttons’. Why does my child need a gastrostomy?
How long does it take for a Gtube stoma to close?
In most cases, when a G-tube is no longer needed, it can simply be removed. The site will slowly close on its own over a period of about two weeks. Usually all that is needed is a bit of gauze to catch any initial leakage.
How long does it take for G-tube hole to close?
Your child’s tract will start to heal and close within hours of removing the feeding tube but it can take more than two weeks to close completely. It will leak during this time. After the tract closes, your child will have a small scar that may look like a dimple or a healed earring hole.
Does PEG tube removal hurt?
The nutrition nurse specialist will then remove the tube for you in the clinic room. Will it hurt? It may be a little uncomfortable. You will be offered a local anaesthetic injection if you feel you need it.
Can a feeding tube cause pneumonia?
As many as 40% of patients receiving enteral tube feedings aspirate the feedings into their lower respiratory tract, resulting in pneumonia. Dislodged or misplaced enteral feeding tubes, high gastric residual volume (GRV), dysphagia, and poor oral hygiene are all possible causes of aspiration pneumonia.
Can you eat solid food while on a feeding tube?
If an individual can eat by mouth safely, then he/she can eat food and supplement with tube feeding if necessary. Eating food will not cause damage to the tube, nor does having a feeding tube make it unsafe to eat.