What is the J point on EKG
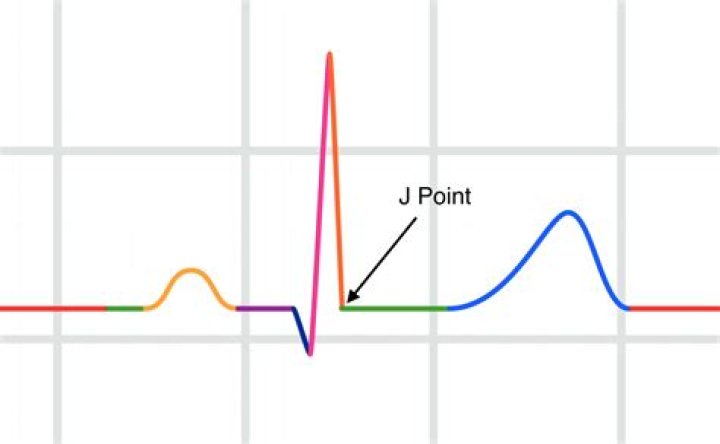
The J point denotes the junction of the QRS complex
What does J point elevation indicate?
The term J-point elevation represents a family of ECG findings. It has been described in several metabolic disorders most notably hypothermia (abnormally low body temperature). Subtle nuances in its pattern may point to other conditions, the most common of which is termed ‘early repolarization’.
When is J point elevated?
The J point of the ECG is at the end of the QRS complex and the beginning of the ST segment. J point elevation can be seen in early repolarization. At times, J point elevation can be ischemic, however, this is somewhat rare.
Which ECG finding is characterized by elevation of the J point?
Early repolarization – UpToDate. The term early repolarization (ER), also known as “J-waves” or “J-point elevation,” has long been used to characterize a QRS-T variant on the electrocardiogram (ECG).What does J point notching mean?
Early repolarization syndrome ER is characterized by prominent J-point on ECG with notching/slurring of distal part of R wave which more or less appears as pseudo delta wave. J notches are known for long time and are actually present in 2–10% of general population.
What is S1Q3T3?
However, the “S1Q3T3” pattern of acute cor pulmonale is classic; this is termed the McGinn-White Sign. Enlarge. A large S wave in lead I, a Q wave in lead III and an inverted T wave in lead III together indicate acute right heart strain.
What causes J waves on ECG?
There are four principal causes of J waves, namely hypothermia, Brugada syndrome, early repolarization and hypercalcemia. Figure 1. Osborn wave (J wave). These waves occur due to hypothermia, hypercalcemia, early repolarization and Brugada syndrome.
What is high take off ECG?
High-takeoff is also known as benign early repolarization. High-takeoff is where there is widespread concave ST elevation, often with a slurring of the j-point (start of the ST segment). It is most prominent in leads V2-5, is usually in young health people and is benign.Which of the following is a historical figure for whom the J point wave was named after in 1953?
History. The prominent J deflection attributed to hypothermia was first reported in 1938 by Tomaszewski. These waves were then definitively described in 1953 by John J. Osborn (1917–2014) and were named in his honor.
Are leads 1 and aVL contiguous?These leads view the high lateral wall of the left ventricle. I & aVL Lateral Wall Leads V5 and V6 are positioned on the left lateral chest and view the lower lateral wall of the left ventricle. Since Leads 1, aVL, V5 and V6 all view the lateral wall of the left ventricle they are considered contiguous.
Article first time published onWhat is Brugada syndrome?
Brugada (brew-GAH-dah) syndrome is a rare, but potentially life-threatening heart rhythm disorder that is sometimes inherited. People with Brugada syndrome have an increased risk of having irregular heart rhythms beginning in the lower chambers of the heart (ventricles).
What is Epsilon wave?
The epsilon wave is a small deflection buried in the end of the QRS complex and represent a delay in the depolarisation of the right ventricular free wall.
Why do athletes get early repolarization?
Early repolarization (ERP) is a common finding in young, healthy, competitive athletes and appears to be a direct result of exercise training. Both ERP and an inferior subtype (originally thought to increase risk of sudden death) increase in prevalence after intense physical training.
Are J Waves bad?
The J wave is a positive deflection in the electrocardiogram (ECG) that occurs at the junction between the QRS complex and the ST segment, also known as the J point.
What does early repolarization mean?
Early repolarization (ER), also recognized as “J-waves” or “J-point elevation”’ is an electrocardiographic abnormality consistent with elevation of the junction between the end of the QRS complex and the beginning of the ST segment in 2 contiguous leads[9,10].
How is J point calculated?
If you go down with the Q wave, up with the R wave, down the S wave and follow the S wave back to the baseline, it will usually pass the baseline. The moment that line goes horizontal, that is where your J point is. You need to find the J point and then measure the distance between the baseline and the J point.
What does an Osborn wave look like?
characterized by a doubling of the QRS interval, and lengthening of the QT interval by three to four times. The T-wave is long and irregular, and usually inverted.
Does pulmonary embolism show up on ECG?
ECG can be normal in pulmonary embolism, and other recognised features of include sinus tachycardia (heart rate >100 beats/min), negative T waves in precordial leads, S1 Q3 T3, complete/incomplete right bundle branch block, right axis deviation, inferior S wave notch in lead V1, and subepicardial ischaemic patterns.
What is cor pulmonale definition?
Cor pulmonale is a condition that causes the right side of the heart to fail. Long-term high blood pressure in the arteries of the lung and right ventricle of the heart can lead to cor pulmonale.
Why does S1Q3T3 happen?
Other common pathological conditions which can cause S1Q3T3 electrocardiographic abnormality are pneumothorax, pulmonary embolism, cor pulmonale, acute lung disease, and left posterior fascicular block.
Who is J Osborn?
John J Osborn (1917 – 2014) was an American intensivist, pediatrician and inventor. Extensive work on hypothermic animals in 1953 allowed him to bear his name on the Osborn wave – what he described as a ‘current of injury’ heralding impending ventricular fibrillation.
How is J point elevation different from ST elevation?
- There is elevation of the J point.
- The T wave is peaked and slightly asymmetrical.
- The ST segment and the ascending limb of the T wave form an upward concavity.
- The descending limb of the T wave is straighter and slightly steeper than the ascending limb.
How do you read and interpret an ECG?
When interpreting the heart rhythm, you should look for P waves, which is a sign of atrial excitation. When every P wave is followed by a QRS complex, the ECG shows sinus rhythm. If the P waves are irregular, sinus arrhythmia is likely present.
How can you tell if an ECG is abnormal?
Abnormal results can signify several issues. These include: Defects or abnormalities in the heart’s shape and size: An abnormal ECG can signal that one or more aspects of the heart’s walls are larger than another meaning that the heart is working harder than normal to pump blood.
When recording an ECG Where is the LA lead placed?
Leads are placed as shown: Right Arm (RA) over the manubrium; Left Arm (LA) over the xiphoid process; and Left Leg (LL) in the standard V4 position (5th ICS MCL).
How do leads look at the heart?
The six chest leads (V1 to V6) “view” the heart in the horizontal plane. The information from the limb electrodes is combined to produce the six limb leads (I, II, III, aVR, aVL, and aVF), which view the heart in the vertical plane. The information from these 12 leads is combined to form a standard electrocardiogram.
Why do we use lead 2 in ECG?
The most commonly used lead is lead II – a bipolar lead with electrodes on the right arm and left leg. This is the most useful lead for detecting cardiac arrhythmias as it lies close to the cardiac axis (the overall direction of electrical movement) and allows the best view of P and R waves.
What does Brugada look like on EKG?
Brugada syndrome is a disorder characterized by sudden death associated with one of several electrocardiographic (ECG) patterns characterized by incomplete right bundle-branch block and ST elevations in the anterior precordial leads.
Can an EKG detect Brugada?
Electrocardiogram (EKG): This test measures your heart’s electrical activity for a short time, using a monitor with electrodes attached to your body. We typically begin with the standard 12-lead EKG, which can usually detect the Brugada pattern of heart rate and rhythm.
Can you live a full life with Brugada syndrome?
It can do, although many people with Brugada syndrome can lead an entirely normal life.
What is Naxos syndrome?
Naxos disease is a recessive association of arrhythmogenic right ventricular cardiomyopathy (ARVC) with wooly hair and palmoplantar keratoderma or similar skin disorder.